If you’re familiar with the term ‘induction of labour’ (IOL) or just ‘induction’ when talking about birth, the chances are you’ve heard about ‘cervical ripening’. Just like the fruit of any tree needs to be ripe before it falls, our cervix needs to be ‘favourable’ or ‘ripened’ before we can birth our baby.
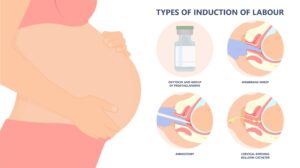
In the induction process there are three steps involved:
- Ripening the cervix,
- Removing the amniotic fluid,
- Making contractions.
Before commencing the induction process a vaginal exam is carried out to determine how ‘favourable’ the cervix is to an induction.
The dilation, (how open the cervix is) effacement, (how thick or thin the cervix is) station, (how low the cervix is in the pelvis) consistency (how soft the cervix is) and position (whether the opening of the cervix is posterior or anterior) are all scored to determine the women’s ‘Bishop Score’.
The higher the score the more favourable the cervix is to an induction of labour.
However, according to research by Kolkman, D,.et al, ‘The Bishop score as a predictor of labour induction success: a systematic review’, American Journal of Perinatology (2013) referred to in Dr Rachel Reed’s ‘Why Induction Matters’ (2018) the Bishop score is not a very accurate way of determining how successful induction of labour will be.
It can, however, inform the maternity care team of what the next best step is to take. For example, some women their cervix may already be favourable enough to skip the ripening part of the induction. If there is need to ripen the cervix for IOL, there are two possible ways to do this; chemically and mechanically.
However, a vaginal exam and or a stretch and sweep can also be considered as a mechanical induction. During a stretch or sweep a midwife or doctor inserts a finger into the vaginal opening to stretch the tissues of the cervix. They will then try and separate the amniotic sac from the lower part of the uterus, to ‘irritate’ the tissues so as to stimulate the release of prostaglandins by the body to encourage cervical ripening. Sometimes when women are having a vaginal exam, they are unaware that they are actually receiving a membrane sweep, which is considered a form of mechanical ripening, as there is a foreign body inserted into the vaginal opening to forcefully stretch tissues and separate the membranes.
The study of routine membrane sweeping by the Cochrane Review found it doesn’t produce clinically important benefits when used to prevent the need for further induction interventions.
Common side effects of receiving a membrane sweep include pain, bleeding from cervix, and irregular contractions and prolonged early labour, which many women are unaware of. An uncommon side effect is accidental rupture of the amniotic sac or rupture of membranes (ROM).
You always have the right to not give consent to vaginal exams and or membrane sweeps. However, if you agree to the induction process vaginal exams are routine and carried out to assess your progress. You always have the right to refuse any interventions or assessments that you do not want.
Let’s talk about the process of ripening the cervix chemically.
Synthetic prostaglandins are used to encourage the tissues of the cervix to soften and stretch and ‘ripen’. Prostaglandins are naturally occurring hormones in our body, and although there are lots of other hormones at play when it comes to ripening the cervix, for IOL, prostaglandins are the hormones that are concentrated on. Synthetic prostaglandins most commonly come as a gel, but also can be given as a pessary which is inserted into the vagina or in an oral tablet form. The gel is inserted high into the vagina as close to the cervix as possible.
After the application of the gel women stay in hospital to be monitored until their baby is born. Routine blood pressure, uterine contractions and the baby’s heartrate will be monitored using a CTG machine. It’s important that women are aware the IOL of labour process can be long, and there isn’t an option to leave after receiving synthetic prostaglandins. There is an assessment of progress six hours after the gel has been applied, and twelve hours after a pessary. If there is not much change to the status of the cervix according to your medical professionals, then another dose of gel will be given, or they may opt to use mechanical ripening instead. If the cervix has opened and progressed, then the woman will move onto the next step in the IOL process which is artificial rupture of the amniotic sac.
The research suggests that receiving synthetic prostaglandins does improve the outcome of IOL. Some common side effects women should be aware of are what medics refer to as ‘prostin pains’ which are sharp pains around the cervix and or uncomfortable uterine cramps. Uncommon side effects are nausea, vomiting, diarrhea, fever and hyperstimulation of the uterus.
Some questions to ask your midwife or obstetrician are:
- What are the rates of caesarean section after receiving prostaglandin gel in their hospital?
- Continuous monitoring, how often will it be?
- Can you move around?
- Are visitors allowed while you’re in the hospital?
- Can you eat and drink as normal?
- How often does hyperstimulation occur?
- How dangerous is this for you and the baby?
- Is there a chance your baby could get distressed if you’re not coping with the prostin pains?
- What could this lead to?
- Can you take pain relief?
- How successful is the gel at causing regular contractions and causing active labour to occur?
- What percentage of women go on to have artificial rupture of membranes and / or Syntocinon (synthetic oxytocin given by drip)?

If a woman is not a suitable candidate for chemical ripening procedures or if chemical ripening has not been successful, the midwife or obstetrician may opt to use the mechanical method of ripening which relies on the woman’s own production of prostaglandins. Mechanical ripening involves inserting an uninflated balloon into the women’s uterus to sit between the amniotic sac and the cervix. It is then inflated with sterile solution and the outer part taped to the inside of the woman’s leg to create traction. The friction of the balloon on the cervix causes prostaglandins to be released. It causes the cervix to stretch which may encourage contractions to start. The balloon will fall out once it has stretched the cervix. The amniotic sac will be ruptured soon after the balloon falls out, before the cervix closes back up.
Common side effects of mechanical ripening include cramping and discomfort; however, women report less discomfort than chemical ripening. Uncommon side effects can be artificial rupture of membranes (ARM) or breaking the amniotic sac, and the balloon getting trapped. Anecdotally, the balloon or ‘Foley’s Catheter’ is causing a lot of mispositioning of babies and cord prolapses.
Some hospitals will allow you to go home once the balloon catheter has been inserted. However, it is worth clarifying this with your maternity care team. Women could ask their care team what the success rate of catheters starting regular contractions and having an unmedicated labour at their hospital is, or how often are they unsuccessful. Another question to ask is about how often they fall out, and in that instance would you have to return to hospital. Can you take pain relief if the cramps are too sore?
Ripening the cervix is the first step in the induction of labour process.
In Rachel Reed’s ‘Why induction Matters’ you can read firsthand accounts of women who have received chemical and mechanical ripening procedures and their thoughts and feelings on how it did, or did not benefit them. It is definitely worth doing your research, getting reputable evidence on success rates of procedures in a relative way that is easy to comprehend for you and your birth partner, so that you can make the best decision for you and your family.
Outside of the medicalisation of ripening the cervix, there is other lifestyle choices that may help promote cervical ripening and spontaneous labour. Historically, women have consumed raspberry leaf tea as a uterine tonic. Anecdotally women and midwives recommend taking raspberry leaf tea to promote effective uterine contractions.
Furthermore, in a trial of 182 women in Iran, women who consumed approximately 75g Medjool dates daily from 37 weeks’ gestation presented at hospital in spontaneous labour with a higher cervical dilatation average, that had a statistically significant difference between the group of women that did not consume dates. The evidence found consuming dates was also effective in decreasing length of the labour process and reduced the need of oxytocin for labour acceleration. It also decreases the chance of postpartum haemorrhaging.
Check out https://addictedtodates.com/ for lots of ways to eat dates! I love to split mine in half, add some peanut butter, dip in chocolate, add sea salt and freeze for later.
Membrane Sweep picture: www.webmd.com
Prostaglandin picture: http://pie.med.utoronto.ca/tvasurg/pe/iol/procedures.html
Foley’s Catheter picture: http://pie.med.utoronto.ca/tvasurg/pe/iol/procedures.html
I’m Cleo Leydon, a student doula at the Doula Training Academy. I live in the northern suburbs of Perth and have a special interest in post-partum care.
Contact me using any of the links below.
Business Name:
A Mama Nua
Business email:
[email protected]
Phone number:
0426 452 105
Instagram:
https://www.instagram.com/a.mama.nua/
Website:
www.amamanua.com (coming soon)